Data extraction and quality assessment
Two independent researchers (CJL, YX) assessed article titles and abstracts, and studies that met the selection criteria were retrieved for full-text evaluation. The literature quality evaluation was also done during data extraction. A third investigator (CSY) helped to address several discrepancies. The first author, publication year, country of study, study type, cancer type, cancer stage, immunotherapy drug, target point of the medicine, TMB detection method, TMB cut-off value, number of patients with high/low TMB, and corresponding data of DCB, ORR, OS, and PFS were extracted into an Excel spreadsheet.
Bioinformatics analysis
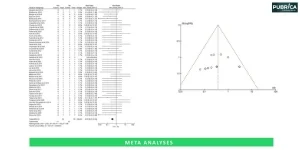
We obtained data on simple nucleotide variation (SNV) from the TCGA database (portal.gdc.cancer.gov/). The workflow type was MuTect2 Variant Aggregation and Masking, and the data format was maf. The TMB of each sample was then calculated using the Maftools R program. The Kaplan-Meier analysis for overall survival was then performed using R software and the Log-Rank to test the TMB of 33 tumours, with the cut-off level set at 70%. The K-M analysis findings are displayed as a forest plot.
Statistical analysis
Stata 16.0 software (Stata Corporation, College Station, Texas, USA) was used for all meta-analyses, and ORR, DCB, OS, and PFS were compared between high TMB and low TMB groups using meta-analysis. For DCB and ORR, RR > 1 indicated that the high TMB group outperformed the low TMB group. For combined HR and 95% CI OS/PFS data, HR > 1 shows that the high TMB group has a worse survival rate than the low TMB group. When I2 was larger than 50%, the random-effect model was employed, and when I2 was less than 50%, the fixed-effect model was utilized. Furthermore, we conducted a subgroup analysis of OS and PFS for various tumour kinds, locations, and TMB detection techniques.
About Pubrica
Pubrica has extensive experience in conducting meta-analysis, a quantitative, formal, epidemiological study design used to systematically assess the results of previous research to derive conclusions about that body of research. Pubrica’s team of researchers and authors develop Scientific and medical research papers that can act as an indispensable tool to the practitioner/authors. Pubrica medical writers help you to write and edit the introduction by introducing the reader to the shortcomings or empty spaces in the identified research field. Our experts are aware of the structure that follows the broad topic, the problem, and the background and advance to a narrow topic to state the hypothesis.